





Toddler’s unusual oral trauma is troubling
A 17-month-old African American girl, with no significant past medical history, is brought to the Pediatric Emergency Department with acute onset of swelling in the floor of her mouth. What's the diagnosis?


Figure 1



Table
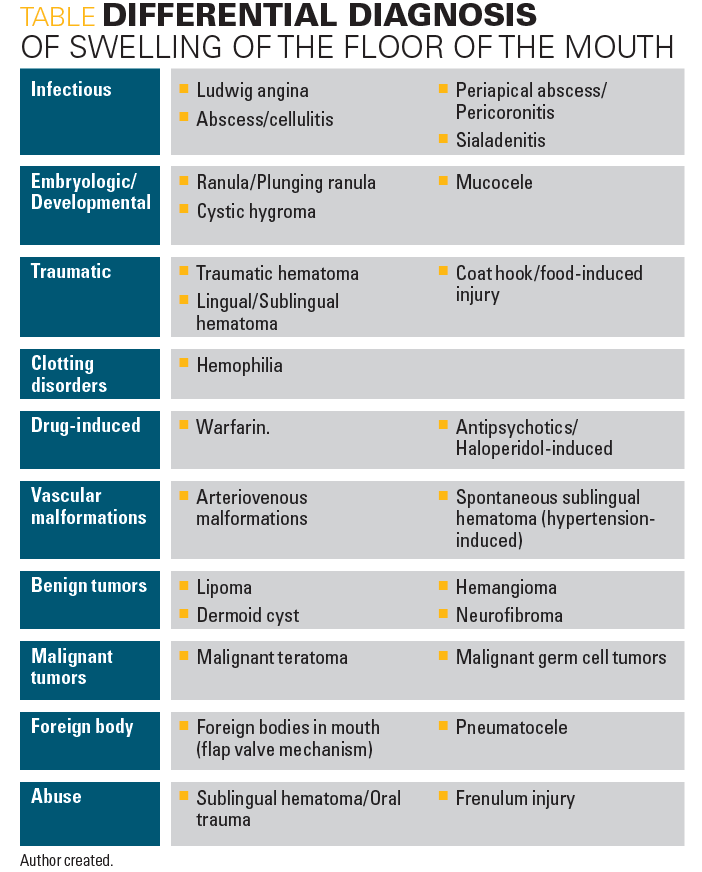


Figure 2



Figure 3



Figure 4

The case
A 17-month-old African American girl, with no significant past medical history, is brought to the Pediatric Emergency Department (PED) with acute onset of swelling in the floor of her mouth. The mother is a reliable historian who denies any recent illness, fever, travel, change in food/new food intake, drugs, or significant injury/trauma.
The girl was in her usual state of health when the mother dropped her at the daycare in the morning. However, after returning home from daycare in the evening, the mother noticed her daughter to be more irritable, drooling, and refusing to eat. The mother also noted a bright red-colored swelling underneath the child’s tongue (Figure 1), which prompted this PED visit. The mother denies any visible rashes, new skin lesions, bleeding, bloody stools, diarrhea, or dark-colored urine.
Exam and testing
On oral exam, bright erythematous, nontender, firm masses were seen underneath the patient’s tongue on both sides of the frenulum area (Figure 1). Mild bleeding was noted from the swelling. Each swelling was 2- to 3-cm in size and located underneath the tongue, appearing firm, noncompressible, and symmetrical in size on either side of the frenulum. Some blood-stained saliva was noted over the swelling. Elevation and bright red-colored swelling under the oral mucosa were consistent with the hematoma noted.
Sublingual caruncles looked swollen and elevated. There was no evidence of any wheezing, stridor, or difficulty with respiration. On examination of the neck, clinicians noted a small swelling in the midline that was soft, fluctuant, and tender to touch, located just behind the chin (Figure 2).
Blood workup showed: white blood cell (WBC) count, 12.5; hemoglobin, 12.4 g; aspartate transaminase (AST)/alanine transaminase (ALT), 33/15; erythrocyte sedimentation rate (ESR), 19 mm/h; uric acid, 1.5 mg/dL; lactate dehydrogenase (LDH), 304 IU/L; C-reactive protein (CRP), 1.04 mg/dL; prothrombin time (PT), 12.8 sec; activated partial thromboplastin (aPTT), 34 sec; international normalized ratio (INR), 1; fibrinogen, 407 mg/dL.
Differential diagnosis
Based on the above results, the possible differential diagnoses of oral cavity swellings in the floor of the mouth are numerous (Table):
LUDWIG ANGINA
Ludwig angina is a bilateral infection of the submandibular space including sublingual and submylohyoid (submaxillary) space. It is characterized by brawny induration of the floor of the mouth with an elevation of the tongue, potentially obstructing the airway. Ludwig angina is up to 90% odontogenic in origin. Other causes are peritonsillar/parapharyngeal abscess, oral lacerations, and mandibular fractures. Fever, neck swelling, bilateral submandibular swelling, and elevation of the tongue are the common mode of presentation. The most common etiologies are aerobes, anaerobes, alpha-hemolytic streptococci, Staphylococcus aureus, and Bacteroides. High-dose intravenous (IV) penicillin, clindamycin, and metronidazole are the best agents for infection. Complications are sepsis, pneumonia, asphyxia, and respiratory obstruction.1
RANULA
Ranula is a mucous retention pseudocyst in the floor of the mouth. It can originate from trauma or obstruction of the sublingual salivary glands, less commonly submandibular/minor salivary glands may be involved. Oral ranulas originate superior to mylohyoid muscle. The intraoral component usually has a bluish color and is typically unilateral, although bilateral swelling can occur. Complete excision of the pseudocyst with the affected salivary gland is associated with the least likelihood of recurrence.2 Cervical/plunging ranulas that penetrate through the belly of the mylohyoid muscle often produce an externally visible neck mass. Posttraumatic ranula will contain mucin in the aspirate. Other modalities of treatment are marsupialization, cryosurgery, and carbon dioxide laser excision.
TRAUMATIC
The oral cavity/neck is a potential target for many injuries. Penetrating injuries secondary to metal bodies/dentures/foreign bodies/metal hooks can be a serious cause of lingual/sublingual hematoma. Few case reports of coat hanger-,3 lobster tails-,4 fishhook-induced oral trauma leading to soft tissue swellings are reported. Infected sublingual hematoma secondary to tongue-tie surgery is reported in the literature as sublingual swelling.
HEMOPHILIA
Approximately 50% to 60% of patients with severe hemophilia (factor level <1% of the factor activity) usually present after oral trauma. It is secondary to dental surgeries, penetrating trauma, and lobsters. Food-induced oral injury can lead to acute bleeds and cause rapid worsening of sore throat, breathing difficulties, and stridor. Prompt treatment with factor 8 concentrates repeated for every 12 hours and close monitoring of vitals and respiratory status are strongly warranted. Early diagnosis and prompt treatment with factor-8 concentrates can protect airways and prevent intubations/surgical management.5
DRUG-INDUCED
Sublingual hematoma is a rare complication of excessive anticoagulation. It can mimic Ludwig angina, often called pseudo-Ludwig phenomenon. Acute onset of sore throat, swelling in the floor of the mouth, drooling, stridor at rest, and difficulty with speaking in a patient on oral warfarin strongly suggests sublingual/submandibular hematoma. Lack of signs of cellulitis and normal inflammatory markers with elevated PT/INR are suggestive of a warfarin-induced hematoma. Sublingual hematomas typically develop quickly and extend posteriorly to involve the supraglottic larynx. Coagulation abnormality can be effectively corrected with fresh frozen plasma, IV vitamin K, and prothrombin complex concentrates.6 Acute lingual/sublingual hematoma secondary to antipsychotic haloperidol drug use has been reported. Acute dystonic reaction involving the head and neck can lead to oral trauma and acute sublingual hematoma.
DERMOID CYST
Dermoid cysts of the floor of the mouth are rare lesions caused by entrapment of germinal epithelium during the closure of the mandibular and hyoid branchial arches. The histological varieties are: epidermoid, if the epidermis is lining the cyst; dermoid, if skin annexes exist; and teratoid, derivatives of 3 germinal layers. A dermoid cyst usually presents as a smooth, doughy, lobular, compressible cystic mass on the floor of the mouth. The cyst lumen is filled with a mixture of desquamated keratin and sebum.7 Complete surgical excision of the lesion using either intraoral or extraoral approach is the best treatment of choice. Magnetic resonance imaging (MRI) of the neck in this patient shows a high-intensity mass on the T2-weighted images of dermoid cyst.
MALIGNANT TUMORS
Teratomas are exceptionally rare tumors in the head and neck region. Neonatal teratomas occur in about 1:20,000 to 1:40,000 live births. Most congenital teratomas are mature or immature ones but they can recur as malignant teratoma after initial surgery.8 Teratomas are tumors containing components of all 3 embryologic germ layers originating from multipotent germ cells. The incidence of malignancy of sacrococcygeal teratoma in neonates is approximately 10% and reaches 100% by age 3 years. Malignant transformation of a teratoma is documented by rapid growth after excision with markedly elevated alpha-fetoprotein (AFP) levels. It can be curable with multi-agent chemotherapy along with complete resection. The residual malignant component can be monitored by serial AFP measurements and complete resection is assured by the decline of AFP to normal after cessation of the chemotherapy.8
FOREIGN BODIES
Foreign bodies are an unusual cause of a slow-growing mass at the floor of the mouth. Fishbones, metal hooks, broken teeth fragments, parts of dentures, pen caps,9 and air rifle pellets are rarely diagnosed and can present with a slow-growing mass in the oral cavity. After the initial injury, the open wound of the floor of the mouth can act as a check valve mechanism that leads to pneumatocele leading to slow growth.
ABUSE
Physical abuse in infants and children is a rare cause of sublingual hematoma. Most common injuries are tears of the lingual frenulum and open wounds of the floor of the mouth, gingiva, and palate.10 Metaphyseal bone fractures, rib fractures, various skin bruises, and retinal hemorrhages are other clinical findings of child abuse. Bleeding diathesis, osteogenesis imperfect, cutis laxa, and Ehlers-Danlos syndrome should be ruled out before the diagnosis of child abuse.
Hospital course
Based on the patient’s clinical history, physical examination, and the acuity of presentation, the clinicians suspected traumatic swelling on the floor of the mouth, probably an acute swelling of sublingual/submandibular salivary glands, as the most common possible etiology. The girl was admitted on the Pediatric floor for close follow-up of the swelling, work of breathing, and oral intake, and close monitoring for any acute worsening of stridor and desaturations. Oral Surgery and Otolaryngology were consulted for further recommendations and management.
On repeat exam after a few hours, clinicians noticed that the color of the swelling changed to dark purplish color (Figure 3). Based on the acuity of presentation, color change of the hematoma, mild bleeding from the swelling, and midline acute tender fluctuant swelling, they strongly suspected oral trauma in this case. As the mother denied any significant trauma, they communicated with the daycare center staff for further clarification and inquired about any possible oral trauma/fall/significant injury during the child’s daycare stay. The staff confirmed that the girl had fallen with a toy (Figure 4) in her mouth/neck while she was running in the daycare.
The Oral Surgery team confirmed final diagnosis as bilateral sublingual hematoma secondary to oral trauma. Oral cavity swellings usually represent engorged sublingual salivary glands with blood/hematoma.
The patient was closely monitored for any worsening of swelling size and development of stridor and drooling. Care continued with warm compressions and a soft, liquid diet as tolerated. She remained stable at room air with stable vitals.
Patient outcome
The patient was discharged in stable condition with instructions for warm compressions and close follow-up instructions with Oral Surgery on an outpatient basis. She was seen after 1 week and her oral swellings were completely resolved without any residual complications or adverse events reported.
References:
1. Srirompolong S, Art-Smart T. Ludwig’s angina: a clinical review. Eur Arch Otorhinolaryngol. 2003;26097):401-403.
2. Zhao YF, Jia J, Jia Y: Complications associated with surgical management of ranulas. J Oral Maxillofac Surg. 2005;63(1):51-54.
3. Cheng J, Kleinberger A, Dunham B, Woo P. Do not hang your coat here. Int J Pediatr Otorhinolaryngol. 2012;76(5):750-751.
4. Kausar H, Gilani JM, Khan OA. No more Doritos and lobster tails: a case report of life-threatening sublingual hematoma. Del Med J. 2009;81(7):255-258.
5. Spindler T, Mc Goldrick N, McMahon J, Campbell Tait R. Spontaneous sublingual haematoma in acquired haemophilia: case report. Br J.Oral Maxillofac Surg. 2017;55(4):e17-e18.
6. Lim M, Chaudhari M, Devesa PM, Waddell A, Gupta D. Management of upper airway obstruction secondary to warfarin therapy: the conservative approach. J Laryngol Otol. 2006;120(2):e12.
7. Lima SM Jr, Chrcanovic BR, de Paula AM, Freire-Maia B, Souza LN. Dermoid cyst of the floor of the mouth. ScientificWorldJournal. 2003;3:156-162.
8. Ueno S, Hirakawa H, Matsuda H, et al. A case of neonatal mature teratoma transformed to malignancy in the neck extending to the mouth floor. Tokai J Exp Clin Med. 2009;34(4):130-134.
9. Uguz MZ, Kazikdas KC, Erdogan N, Aydogdu V. An unusual foreign body in the floor of the mouth presenting as a gradually growing mass. Eur Arch Otorhinolaryngol. 2005;262(10):875-877.
10. Kudek MR, Knox BL. Sublingual hematoma: when to suspect child abuse. Clin Pediatr (Phila). 2014;53(8):809-812.
















11-year-old boy with testicular pain and rash
January 19th 2024An 11-year-old boy presented to the emergency department complaining of left testicular pain for 2 days, described as intermittent and stabbing, which ranged between 5 and 8 of 10 in intensity. Read the full case to see if you can correctly diagnose the patient.

Newborn with midline neck lesion
December 21st 2023A 4-day-old boy with a midline neck lesion was born at term by normal vaginal delivery. After birth, mid line lesion had the configuration of a linear cleft with a cephalocaudal orientation, extending from the level below the hyoid bone to the suprasternal notch with a length of 2.5 cm and a width of 0.5 cm. What's the diagnosis?

A 13-year-old girl with well-demarcated rash on back and chest
October 19th 2023A healthy 13-year-old girl presented with a 1-month history of an asymptomatic, well-demarcated rash on her back and upper chest. The eruption consisted of discrete, dark brown papules that coalesced into large, flat-topped plaques with mild superficial scale and accentuation of skin markings. What's the diagnosis?

Suspicious facial swelling in a 22-month-old girl
October 11th 2023A 22-month-old female patient with sickle cell disease on folic acid and penicillin prophylaxis with a 3-day history of nasal congestion, rhinorrhea, fever and decreased oral intake presents to the emergency department (ED) for acute facial swelling noted when she woke up from a nap. What's the diagnosis?

Friction-induced blistering on a child’s feet
July 14th 2023You are called to the hospital nursery to evaluate a healthy full-term newborn boy who developed painful flaccid blisters and erosions on the tops of his feet and ankles shortly after birth. His mother had a history of similar recurrent skin lesions that healed with scarring. She also had oral and gastrointestinal tract involvement. What's the diagnosis?

