





An Honor for Our Own Dr Leung
A city's favorite son might have a street named after him. It is common for Broadway theaters to be named for famous actors and actresses. An equivalent distinction for a physician is to have a condition named after him or her. Alexander K. C. Leung, MD, long-time member of the editorial board of CONSULTANT FOR PEDIATRICIANS, recently joined the ranks of those physicians who have been so distinguished. Dr Leung is clinical associate professor of pediatrics at the University of Calgary and pediatric consultant at the Alberta Children's Hospital in Calgary.
A city's favorite son might have a street named after him. It is common for Broadway theaters to be named for famous actors and actresses. An equivalent distinction for a physician is to have a condition named after him or her. Alexander K. C. Leung, MD, long-time member of the editorial board of CONSULTANT FOR PEDIATRICIANS, recently joined the ranks of those physicians who have been so distinguished. Dr Leung is clinical associate professor of pediatrics at the University of Calgary and pediatric consultant at the Alberta Children's Hospital in Calgary.
Hegde-Leung syndrome, whose hallmarks are acral anomaly, aplasia of the right pectoralis major muscle, and renal anomaly, was identified by Dr Leung and his colleague, Hardally Hegde, MD, after they had noted this distinctive combination of anomalies in several patients over the years and read about similar cases in the literature.
The first patient to come to their attention, back in the late 1970s, was a 9-year-old girl who, in addition to aplasia of the pectoralis major muscle, had ipsilateral agenesis of the kidney (Figure 1). The second patient was a 69-year-old man who had absence of the sternal portion of the right pectoralis major muscle, absence of the right supraspinatus muscle, and ipsilateral duplication of the urinary collecting system. With their suspicion piqued, Hegde and Leung searched the literature and found 3 additional cases of patients with aplasia of the right pectoralis major muscle and various renal anomalies.1 The two proposed to designate such a combination of anomalies the "acro-pectoro-renal field defect."

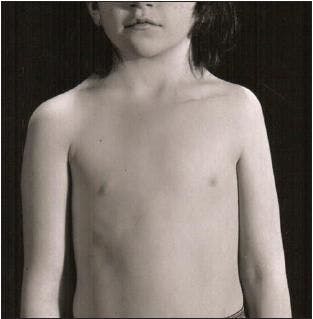
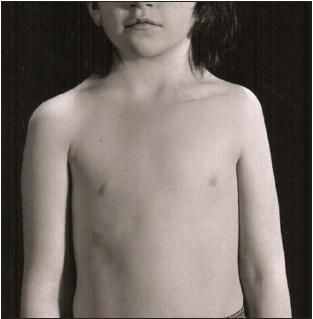
Figure 1 – The flatness in the right mammary and inframammary areas in this girl is the result of the absence of the lower portion of the right pectoralis major muscle. Other anomalies observed in this patient included winging, hypoplasia of the ipsilateral scapula, cervical encephalocele, and short webbed neck resulting from fusion of hemivertebrae. Subsequent ultrasonographic examination revealed agenesis of the right kidney. This patient was the first in whom Dr Hegde, along with Dr M. H. Shokeir, diagnosed acro-pectoro-renal field defect.
At this point they postulated that this constellation of anomalies represented a new polytopic developmental field defect but probably not a syndrome. They suggested that its origin was a vascular injury of some sort during the sixth or seventh week of embryogenesis. Over the years, more cases continued to be reported.
In 1995, Drs Hegde and Leung and Dr William Lane M. Robson encountered a patient in whom the renal anomaly occurred on the contralateral side. This newborn male infant had hypoplasia of the right hand and absence of the first 3 fingers (Figure 2), absence of the sternocostal portion of the right pectoralis major muscle, and contralateral ureteropelvic junction obstruction.2 This "discovery" led to an expansion of the criteria for acro-pectoro-renal field defect.



Figure 2 – The hypoplastic hand shown here, on which 3 fingers are absent and the fourth is only rudimentary, is that of a male infant who also had a deformed right chest wall, hypoplasia of the right nipple and areola, and cupping of the left ear. Examination revealed contralateral ureteropelvic junction obstruction. This was the first case in which Drs Hegde, Leung, and Robson noted renal anomaly on the side opposite that on which agenesis of the pectoralis major muscle was noted.
By 2004, at least 17 cases of the defect had been reported. Recently, other authors began referring to acro-pectoro-renal field defect as "Hegde-Leung syndrome." And so a new medical eponym was born-as most are, through a consensus that is the result of a natural evolution in educated usage.
Although Hegde-Leung syndrome is quite rare, Dr Leung notes that his work on it has yielded a valuable "take-home" message to practicing pediatricians "in the trenches"-that is, renal ultrasonography should be ordered for any child in whom aplasia of the pectoralis major muscle has been discovered.
References:
1.
Hegde HR, Leung AK. Aplasia of pectoralis major muscle and renal anomalies.
Am J Med Genet.
1989;32: 109-111.
2.
Hegde HR, Leung AK, Robson WR. Acro-pectoro-renal field defect with contralateral ureteropelvic junction obstruction.
Clin Genet
. 1995;47:210-213.

















